parapox virus:
better known as cowpox and poxvirus, consists of various open reading frames (ORFs) some of which overlap with “monkeypox.”

In “sars-cov-2” some people will express five ORFs.
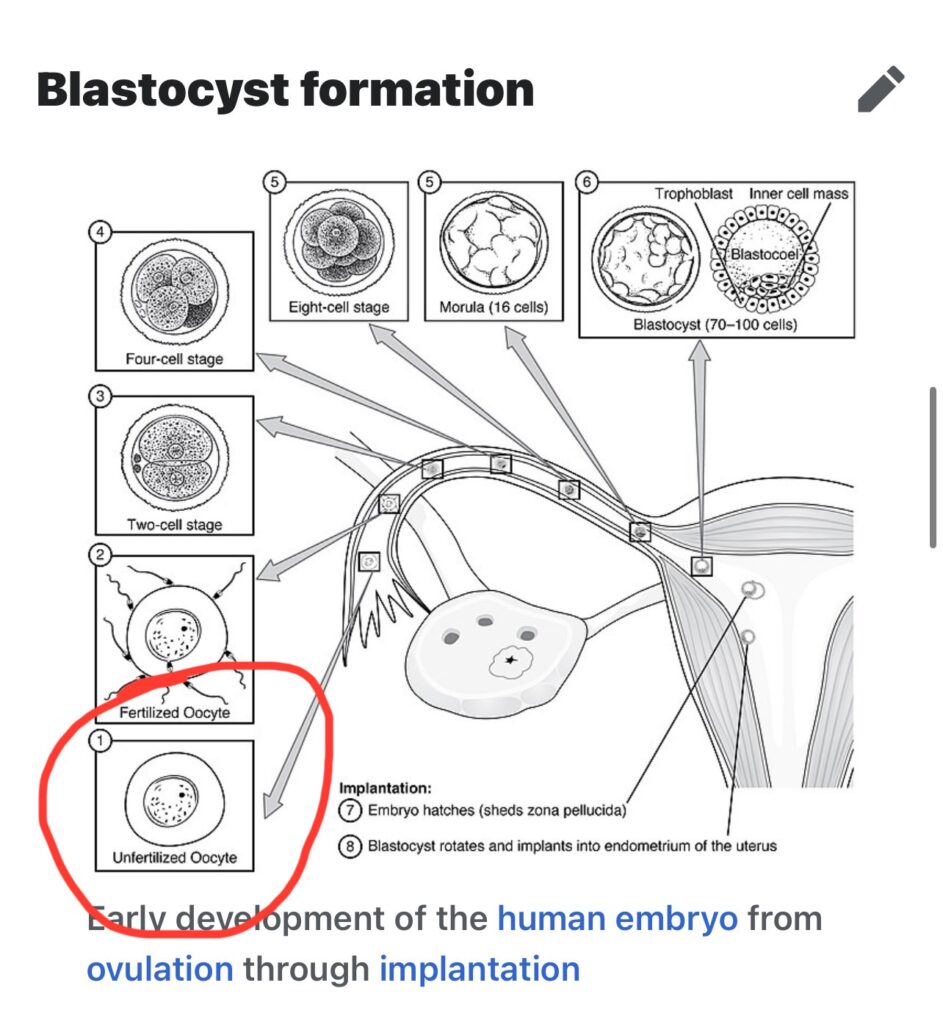
The people who express ten ORFs are vanished twins or twins in situ.
Furthermore, while again diverging from the biblical Job (20:14 His food in his bowels turns into asps’ venom within him) the lack of food allergy observed in this rare disease associated with the overproduction of an antibody associated with allergy actually led to the identification of a potential therapeutic target—inhibition of STAT3—to treat severe allergy in the general population.
Eh they’re not “asps” they’re “just” vestigial blastocytes , in situ twins, and it’s not “asps venom,” it’s rectal endometriosis. This is what China and Iran were looking for in peoples asses.
This is what the gods are listening to or harvesting in these images. They were depicting this 230,000 years ago:
The “mystery illness” I had in Florida in 2019, when I wrote this entry on or around November 6, 2019 in Miami, was likely “endometriosis” just after the “great dimming” of Betelgeuse in October of 2019.
Officials in China have used anal swabs to test people it considers at high-risk of contracting the illness, including residents of neighborhoods with confirmed cases as well as some international travelers, according to AFP.
Tests using anal swabs can avoid missing infections as viral traces in fecal samples or anal swabs could remain detectable for longer periods than in those from the respiratory tract, Li Tongzeng, a respiratory diseases doctor in Beijing, told state TV recently.
Stool tests also may be more effective in detecting infections in kids as their waste carries a higher viral load than adults, researchers at the Chinese University of Hong Kong said in a paper published last year.China’s National Health Commission said in an online post that in some cases, the deadly bug can be more easily detected in anal samples than in throat and nasal samples.
https://nypost.com/2021/02/25/china-reportedly-gave-american-diplomats-anal-covid-19-tests/
You have blastocytes in your foreskin that are immune to the plague so they snip that off at birth.
The females live after the plagues.
By design.
They have blastocytes in their unfertilized eggs.
Given enough time with this condition now you’re “white” and “stole” your ancestral homeland and here’s someone telling you who “deserves it.”
And males such as Job, who likely had vestigial blastocytes from a vanished or in situ twin, also survive the plagues.
Unlike his ten sons and daughters who perished.
It was said that Job lived 210 years; this is inferred from Job 42:16, where it is said that he lived 140 years after his recovery. It is said also that the whole world mourned Job’s death.
https://en.wikipedia.org/wiki/Job_in_rabbinic_literature
When it happens to Job in your bible it’s called “Job’s Syndrome” and it’s a “test of his faith” as he’s covered in sores.
But noooo, I need my dick chopped and “vaccines.”
I believe that “trans” may have had a vanished or in situ fraternal twin of the opposite gender.
this is something some of you would know as “Becoming X” or “becoming.”
Or the one who was, who is, and who is yet to come.
Mine was/is male.
Kat used to vacuum .. well.. no one will believe me .. but yeah she would do that once every few years whether it needed it or not .. singing “I’m a zygote, I’m a zygote, I’m a zygote” … like in family guy: “I’m a tumor I’m a tumor I’m a tumor.”
Though you and your “plagues” and your peculiarities are referred to repeatedly in the Bible, associated with people who God favored or anointed, there are people who will still call you an abomination for experiencing the same things.
Job heard “satan” and “god” quarreling.
And all throughout my childhood, Jobs ordeal was beautiful and a testimony to his faith his god and overcoming the Adversary.
But I “need schizophrenic meds.”
And my candidisis is “aids”
And I “deserved it because I’m gay.”
I have a fun one for you: The “electrostatic blanket” I described sounds a lot like Phillip K Dick’s “Scramble Suit” in his book A Scanner Darkly.

I’m not going to stop there, either:
We were told not to forget or stop speaking of many languages, many races, many people or what happened when the “tower of Babylon” (whatever that was, probably an ancient surveillance apparatus like conventional satellites are today: remember that time is dilated underground and time is compressed at altitude/in space) fell, well, the people who survived that probably had endometriosis or shed their in situ twins, and started having changes in skin color or other traits that had been suppressed due to competing genetics , so called “retroviruses”. etc that were resolved after some kind of massive solar flash or solar/corona event that occurred in the “tower of Babylon” incident and epoch.
The blacks keep saying theyre going to develop “superpowers” after some kind of solar flash aaahhahhahah I hope you turn white, Kylon! JUST PLAYING!

I have repeatedly said plagues and epidemics appear during solar maximums and that the UN Agendas are all timed for these events- they know this.
John receives word that he must prophesy again about many people and nations and languages and kings.
Then I was told, ‘You must prophesy again about many peoples, nations, languages, and kings.’
Revelation 10:00
Learning from Job: A Rare Genetic Disease and Lessons of Biblical Proportions
Joshua D. Milner, M.D.
Abstract
Dominant negative mutations in STAT3, a critical signaling molecule and transcription factor in multiple organ systems, lead to a rare monogenic disease called the STAT3 loss-of-function, autosomal dominant hyper-IgE syndrome (STAT3LOF AD-HIES). The original name for this syndrome, Job’s syndrome, was derived from the observation that patients had a propensity to develop skin boils, reminiscent of the affliction cast upon the biblical Job. Many fascinating observations have been made regarding the pathogenesis of the disease and the role STAT3 plays in human health and disease. Additionally, quite a few phenotypic descriptions from the Book of Job are similar to those seen in patients with STAT3LOF AD-HIES, beyond just the boils. This complex multisystem genetic disorder is a challenge clinically and scientifically, but it also brings into question how we approach genetic syndromes beyond just the technical aspects of research and treatment.
Keywords: Hyper-IgE, infection, monogenic disease
INTRODUCTION
Studying rare genetic syndromes can provide invaluable insight into fundamental pathways in health and disease, beyond the benefit to the rare patient affected by such disorders. In years past, such novel syndromes tended to be named either to correspond to a specific symptom commonly associated with it (e.g. familial Mediterranean fever) or after the name of the physician(s) involved in the initial description of the disorder (e.g. Wiskott–Aldrich syndrome). One unique outlier not initially named by any of these criteria is Job’s syndrome. In 1966, Ralph Wedgwood and colleagues in Seattle encountered two sisters with a significant, long-standing history of skin boils, which, interestingly, were not associated with the signs of inflammation expected from such infections and were hence described as “cold” abscesses. The decision was made to call the disorder Job’s syndrome, recalling the boils afflicted upon the biblical character Job as a test that emerged from an exchange between G-d and Satan. (2:7 So Satan went forth from the presence of the LORD, and smote Job with sore boils from the sole of his foot even unto his crown.)1
This disorder is extremely rare—there may be fewer than 1,000 people in the world affected—but it has been studied extensively ever since because of the complicated symptoms these patients can develop, and for the insight the underlying cause provides into the human immune system, musculoskeletal and circulatory systems, and more.
Since the initial naming, two substantial findings over the years have provided additional names. The first was that IgE—the antibody most tightly associated with allergic reactivity—is markedly elevated in these patients,2 prompting the name “the hyper-IgE syndrome” or the “autosomal dominant hyper-IgE syndrome.” Interestingly, in part because the observation of high IgE was made by legendary pediatric immunologist Rebecca Buckley, for some period of time the disease bore her name, “Buckley syndrome.” Subsequently, however, multiple syndromes with presentations and inheritance patterns distinct from Job’s syndrome have been identified which lead to such IgE elevations, including even another autosomal dominant one (CARD11 mutations3), leading to the need for a more precise term. The second was the discovery that dominant negative mutations in STAT3, a critical transcription factor for numerous cellular signaling pathways, underlie the disorder.4,5 Subsequently gain-of-function mutations in STAT3 were identified in patients with autoimmunity and lymphoproliferation,6–8 necessitating the clarifying title “STAT3 loss-of-function” (STAT3LOF). With its negative connotation of affliction with a disorder of biblical proportions, the name Job’s syndrome is now less commonly used; the more descriptive STAT3LOF AD-HIES (STAT3 loss-of-function, autosomal dominant hyper-IgE syndrome) better captures the disease. It is noteworthy that the progression of terms—from a malady of biblical dimension, to a description of a remarkably abnormal clinical finding not necessarily central to the disease, to the genetic root cause of the disorder—mirrors in many ways how we have evolved in our understanding of such diseases in general.
The title Job’s syndrome was perhaps more prescient than initially recognized. Beyond the boils and infections which were noted initially, many of the symptoms with which the patients present can be found—without too much stretching of the imagination—in the text of the Book of Job, either from Job’s descriptions of his fate or in the descriptions by those who came to console him.
THE PHENOTYPE OF STAT3LOF AD-HIES AND PATHOPHYSIOLOGIC MECHANISMS
Patients with STAT3LOF mutations develop chronic mucocutaneous candidiasis (CMC) throughout their lives and can get skin rashes which resemble atopic dermatitis from birth, differing from classic atopic dermatitis. (2:4 And Satan answered the LORD, and said: “Skin for skin, yea, all that a man hath will he give for his life.”/7:5 My skin is broken and festering.) Eosinophilic esophagitis—associated with difficulty swallowing, impacted food (20:15 The riches he swallows he vomits/20:18 He will give back the goods unswallowed; The value of the riches undigested), and resulting in refusal to eat at times (6:7 I refuse to touch them; They are like food when I am sick)—has been observed as well.9
The non-immunologic symptoms in these patients include joint hypermobility (31:22 May my arm drop off my shoulder), failure of childhood teeth to fall out (13:14 How long! I will take my flesh in my teeth/19:20 I escape with the skin of my teeth), easily fractured bones (2:5 But put forth Thy hand now, and touch his bone and his flesh, surely he will blaspheme Thee to Thy face./31:22 My forearm break off at the elbow) possibly due to increased bone resorptive activity (30:17 By night my bones feel gnawed),5 scoliosis, characteristic facies including a broad nasal bridge and asymmetry, and aneurysm formation, primarily in the coronary arteries (17:11 My days are done, my tendons severed, The strings of my heart).9
Perhaps the manifestation with the greatest morbidity is lung disease, principally caused by Staphylococcus aureus infection, which can lead to cavitating lung cysts (pneumatoceles) and bronchiectasis (9:18 He does not let me catch my breath). Other infections patients can encounter include CMC, recurrent pneumococcal and Gram-negative respiratory tract infections, and invasive fungal diseases.9
Primary viral infection does not appear to be a significant issue, but herpesvirus reactivation in the form of Varicella Zoster Virus and chronic Epstein–Barr virus viremia have been observed. The precise mechanisms for infections continue to be elucidated. The candidiasis appears to be due to the lack of a specific type of cytokine needed for anti-candidal responses, IL-17,10–12and some of the bacterial infections may be explained by B-cell defects in maturation and memory development, which in some patients is prevented by intravenous immune globulin.13,14 In general, it appears that patients have difficulty with maintaining the long-term cellular “memory” needed to normally keep certain infections at bay, thereby allowing such infections to persist or recur abnormally.13,15
STAT3LOF AD-HIES AS A PARADIGM FOR ALTERING THE BALANCE OF PROTECTION FROM INFECTION AND SUSCEPTIBILITY TO INFLAMMATION
On another level, some of the deeper messages in the biblical text bear some similarities to this unique disorder as well, as will be outlined below. Of course, no one would really try to claim that Job actually had Job’s syndrome. (Of note, a colleague of mine once circulated a remarkably realistic-appearing article from a prominent journal claiming to have found bones in an ossuary in Ashkelon with Job’s name on it that tested positive for a known mutation in STAT3; the text was sent on April 1—or April Fool’s Day.)
The adult onset of Job’s symptoms (as opposed to infancy, which also would have been fatal prior to intravenous immune globulin and antibiotics), and the lack of any noted family history of this dominant disorder makes this congenital disease a highly unlikely cause (the tragic death of his children, again after infancy, is due to attacking groups and to a mysterious “wind”). Scholars in the medical literature have proposed everything from kidney disease,16 to primary dermatologic disorders,17,18 to poisoning,19 to psychiatric disorders,20,21 and have taken to psychoanalyzing Job as well.22–25 Nonetheless, it is valuable to ponder ancient encounters with disease and affliction, and contrast them to the modern ways that we understand, perceive, and deal with genetic diseases. Like the affliction of Job, these diseases are well beyond the control of those affected and lead to tremendous challenges and suffering. Scholars have focused on the “doctor–patient relationship,” as it were, between Job and the various other characters in the book, and on the process of grieving and consolation in general,26–29 and today, in an era when the underlying genetic cause of biological differences and/or disease can frequently be identified (sometimes even before a symptom appears), an oft-ignored issue arises: Whether or not a cure is found, how is the affected individual and his/her caregivers to understand and cope with such a rare disease that is fated from birth? Even when the precise genetic cause is identified, does it provide any more solace?
What brings Job the most solace is a lecture from G-d at the very end of the book. It is fundamentally about how humans and other living beings cannot possibly know or control all the various differences or “mistakes” that are made that lead to good and bad outcomes in nature. In one instance G-d points out (Job 39) regarding the ostrich that “14 She leaves her eggs on the ground, Letting them warm in the dirt, 15 Forgetting they may be crushed underfoot, Or trampled by a wild beast.” As the nineteenth-century biblical commentator Malbim points out, this is contrasted to the stork that flies high but lays few eggs which must be guarded more carefully, “18 Else she would soar on high, Scoffing at the horse and its rider.”
One could interpret this point as G-d trying to explain to Job that in addition to the basic lack of insight into nature, an insight that he will never really have, there will always be a tradeoff between advantages and disadvantages—soaring freedom and risk for disaster—which are exceedingly difficult to understand, and therefore the particular set point of risk for any individual will always come into question. STAT3LOF AD-HIES is not the only rare genetic disease with such tradeoffs (the causal mutation in Sickle cell anemia protects the unaffected carriers from malaria, and theories have been proposed that unaffected carriers of the gene causing Tay–Sachs might be more intelligent), but it is a good example of one, and certainly makes anyone affected wonder: “why me?”
Amongst the tradeoffs noted in STAT3LOF AD-HIES, a major one is the lack of damaging inflammation at the cost of increased infection. The abscesses seen in these patients fail to express cardinal signs of inflammation such as swelling (tumor), heat (calor), redness (rubor), and pain (dolor)—a potential departure from the biblical Job (“2:8 and he sat among the ashes …”, which is interpreted by some to mean not just mourning but the need to cool off his “hot” wounds). In addition, while the patients fracture bones easily, they tend to not realize the extent of their injury. The pneumonias that occur are not associated with the level of discomfort one might expect until they are quite severe, and in fact are sometimes only diagnosed with grossly abnormal CT scans—necessitating careful imaging studies even in the absence of illness. It is also interesting that, despite having such high levels of allergy-associated IgE, patients are relatively protected from severe allergic disease and anaphylaxis. The mechanism appears to be a requirement for normal STAT3 function in mast cell degranulation and endothelial responses to histamine, and in fact in vivo treatment of mice with STAT3 inhibitors prevents anaphylaxis.30,31 Furthermore, while again diverging from the biblical Job (20:14 His food in his bowels turns into asps’ venom within him) the lack of food allergy observed in this rare disease associated with the overproduction of an antibody associated with allergy actually led to the identification of a potential therapeutic target—inhibition of STAT3—to treat severe allergy in the general population.
Further, patients with STAT3 deficiency might have been predicted to have colitis, since patients with loss of the IL-10 receptor—which signals through STAT3—have severe early-onset inflammatory bowel disease (IBD).32 However, unlike the biblical Job (30:27 My bowels are in turmoil without respite), they do not, potentially due to the lack of Th17 cells.10 Study of STAT3LOF AD-HIES patients first demonstrated the consequence of a lack of these cells, namely CMC, but their absence may also explain why IBD and perhaps other types of autoimmunity are absent. Indeed, blocking IL-17 is an effective treatment in a variety of inflammatory and autoimmune conditions.33 Despite the heart disease caused by aneurysm, the coronary arteries in these patients are relatively (though not completely) protected from the plaque and atherosclerosis that might be expected.34–36 One also wonders if joint hypermobility, which on the one hand can be associated with chronic pain and arthritis, might nonetheless confer an advantage to individuals in certain scenarios.
It is indeed quite possible that some of these paradoxical protections—from certain types of pain, inflammation, atherosclerosis, allergy, and autoimmune disease—might well confer an advantage, as opposed to reflecting further disease. They represent a different set point for the tradeoff between excessive inflammation and excessive infection. While the disease can be quite severe in many patients, early management can, in a substantial subset of these patients, prevent many of the worst symptoms. Finally, once past their adolescent years, patients who have been able to manage their infections earlier in life tend to see a reduction in infection, and even in IgE levels. There can be patients who are “restored” (42:10 And the LORD changed the fortune of Job, when he prayed for his friends; and the LORD gave Job twice as much as he had before) as it were, but not without the scars of their ordeal, and not without future suffering or risk of disease.
APPROACHING GENETIC SYNDROMES: DO WE ADEQUATELY ADDRESS THE AFFECTED PERSON AND THEIR CONCERNS IN THEIR ENTIRETY?
In proving G-d correct over Satan, Job curses the day he was born (perhaps when a congenital issue would first manifest?) but does not curse G-d. Nonetheless, his “friends” who come to console him do anything but. Much of their rebuke could be summarized as: “Buck up, who are you to complain? You probably deserved it because of some sin, and repentance will be the cure.” In truth there could be no consolation for his loss, only a restoration of faith and property, which happens after Job comes to terms with his relationship to the divine (and in a universalist setting, perhaps that which is beyond his reach or control) and to others (his visiting friends with whom he has a reconciliation).
It may never be fully understood what about G-d’s lecture helped Job to get there. Such insight will never fully console or restore anyone, but at least it may help to reframe the issue for all of us—from patients to impacted loved ones, to health-care providers—in an era of unprecedented technological advances which get at the genetic and biological causes of myriad afflictions, often a long time prior to any practical treatment based on the finding.
In an essay about the dimensions of palliative care in suffering patients, Theodore Fleischer uses the Book of Job as a model for dealing with severe illness and suffering in the face of modern technological advances which, in his view, fail to address a dimension important in many of those with diseases: “Why do I have this?”27 While his essay was about end-of-life palliative care, the analysis could well be applied to the complexities of being born with a rare multisystem congenital disorder. Indeed, the research into how to try and cure the suffering is critical. But faith in a cure, or, believe it or not, the cure itself is probably not enough for many. Noting that the visitors to Job repeatedly harped on his complaining and cursing of the day he was born, and told him that sin—which Job felt he did not commit—was the reason he was afflicted, Fleischer writes:
Solutions that utilize only techniques to manage pain ignore the patients’ need to interpret their experiences of suffering. Like the religious solution [repentance] rejected by Job … this topical remedy falls short of providing an answer to the patients’ search for a stance that allows them to cope with the depth of their suffering. Palliative care cannot substitute for meaning.27
And later he notes:
The story of Job illuminates dimensions of suffering that are as relevant today as they were in biblical times. All who suffer need to interpret their suffering. Job rejected a solution that failed to acknowledge the depth of his disorientation and the abyss that separated him from God and his fellow humans. Instead, he found a solution in renewed covenantal relationships with God and the human community. Only then could Job reclaim his suffering.27
Regarding patients themselves who struggle with these issues:
When they refused to be distracted by technological solutions and instead sought to understand the role of suffering in their lives, they were finally able to truly express their autonomy.27
As a final note, a word to the wise from Job himself for those, like his visitors, who try too hard to approach this problem without truly understanding all the dimensions of suffering an affected person might have: “13:4 But you invent lies; All of you are doctors for idols.” Understanding the technical dimensions of genetic diseases in order to improve the physical health of affected patients is of course critical, and in this era such diseases will be genetically solved at an extraordinary rate. However, care must be taken not to ignore the more fundamental questions of what it means to be born with a “mutation,” and to understand that the affected individual has been the made the subject of a different set of tradeoffs of gain and loss of function of different pathways inherent in any biological system in balance that sets them apart and leaves them wondering why. Caregivers should have that in mind when approaching such populations.
Acknowledgements
This work was supported by the Intramural Research Program of the NIAID, NIH. English translations are based on the English text in sefaria.org and the Jewish Publication Society 1917 Bible translation. The author thanks Aliza Sperling and Bayla Jacobson for critical readings of the manuscript.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5796737/
Leave a Reply